“Damn the things we must survive to survive.” –Pat Parker to Audre Lorde in a letter dated January 4, 1988, from Sister Love: The Letters of Audre Lorde and Pat Parker 1974-1989
It’s mid-August, and I’m done with chemo. I feel like I have enough distance from my last cycle to look back on that phase of treatment and assess what it cost me, where I am, and where I’m going. I had intended to write about each cycle as it happened, describing my body’s reaction and comparing it to others’ experiences, which were so useful to me in deciding whether or not to do chemo and knowing what to expect. But I didn’t have the will or energy to do so, and the anticipatory nausea became so strong, I don’t think I could have gotten through a paragraph without vomiting. By cycle 6, I felt like I was just hanging on by my fingernails, and I feel like I wouldn’t have survived a seventh cycle.
For me, the worst part was the anticipatory nausea. In so many of the accounts I read of others’ chemo experience, the person said the right anti-nausea meds took most of the nausea away. This wasn’t my experience at all. The anti-nausea meds (and I had three different kinds) didn’t even make a dent in the anticipatory nausea.
Going into chemo, I didn’t even know anticipatory nausea was one of the primary forms of nausea chemo patients experience. At cycle 3, I think it was, I told my oncologist, it’s weird I’m nauseous today because I haven’t been since day 8 of the last cycle, so I guess this must be in my head? He said oh yes, this is anticipatory nausea, and explained that my amygdala had made the connection between the assault on my body (by the chemo, which are cytotoxins) and the cancer center. He said there’s nothing a person can do to avoid this connection from being made, and that a trigger for one of his other patients is the McDonald’s sign near the cancer center.
My anticipatory nausea has many triggers, the strongest of which is the saline (*gag*) used to flush my port and in between different chemo drugs (*still gagging*). There’s a preservative in the saline (*gag*) that some people can taste or smell as it’s being injected. A lucky few taste lemons. I taste what I imagine skunk spray would taste like, and the smell of skunk is another trigger. This makes car drives interesting, and I swear to God, how many skunks does this state have, and do people go out of their way to hit them?!
The nails of my anticipatory nausea got sharper and sharper with each cycle, so that by the sixth one, I couldn’t fight the dry heave whenever the nurse set saline (ugh) on the table. I tried to maintain control by sucking on a mint (which is also now a trigger, any mint, in any format, goodbye peppermint mochas, and don’t even open a gum wrapper around me) during the saline (oh god) injections, and when that stopped working, cinnamon discs, which weren’t as effective. I also had to switch from the mango popsicles (*GAG*) I sucked on during the injection of the doxorubicin (done to avoid mouth sores) to just ice starting with chemo cycle 4, and I just can’t even with anything mango. Other triggers include simply thinking about the cancer center/treatment/chemo, driving in the direction of the cancer center, seeing anyone with an IV or even seeing a bag of saline, the smell of my chemo bag, corn dogs (I had this for lunch once during chemo), anything ginger (and I LOVED ginger before chemo, especially Bundaberg ginger beer), and to a lesser extent, Gatorade and even water (and you have to drink A LOT of water during chemo).
Another hard part of chemo, for me, was the prednisone. I had to take 5 tablets a day for the first five days of each chemo cycle, and the pill is so bitter (like, next level bitter) and large that it’s like wrestling an octopus to get each one down. I once gagged so hard that I spit up all the water I’d taken with the pill, but thankfully, the pill stayed down. Iced tea made swallowing the pills much, much easier, but I still felt exhausted afterwords from the gagging. And the prednisone made me uncomfortably warm and caused my face to flush and my heart to pound. Other cancer patients describe prednisone rage, but it actually made me weep (and I do mean weep) at the silliest things. Harry Styles’ music video for “Falling,” for example. Not having rice and beans with sour cream on top when the craving hit. It also made me gain about 23 pounds.
And of course, there was the fatigue. Which led to the constant, can’t-even-tolerate-your-nonsense grumpiness of cycles 5 and 6.
My treatment team has been absolutely wonderful so far, but there were things they could have done differently to make my experience a little easier. For example, two of my most important and nerve-wracking appointments–the one where I got the results of my mid-chemo PET scan and the one where I got the results of my post-chemo PET scan–were with my oncologist’s PA, rather than my oncologist, who didn’t have an opening on those days. I would have preferred to meet with his PA every other appointment as long as I could meet with him for those two.
It also would have made my post-chemo PET scan results easier to digest if my oncologist had been less enthusiastic about my mid-chemo PET scan results. The next time I met with him following my appointment with his PA to go over the mid-chemo results, he told me I had experienced a “complete response” and that I wouldn’t have to do radiation or two extra cycles of chemo. I only shared this news with one or two people, and I didn’t celebrate and tried not to get my hopes up because I don’t like to count my chickens before they hatch. Also, based on the pathology report, I knew my cancer was likely to be resistant to chemo, and that if it rebounded, it often happens during the last cycles of chemo or shortly after. I didn’t want to give my loved ones another bad-news blow if the post-chemo PET scan wasn’t what my oncologist expected. And it wasn’t. The SUV max was slightly higher than the mid-chemo PET scan, which forced me back to that place cancer loves so much: impossible decisions. Despite the risks, the PA recommended radiation therapy.
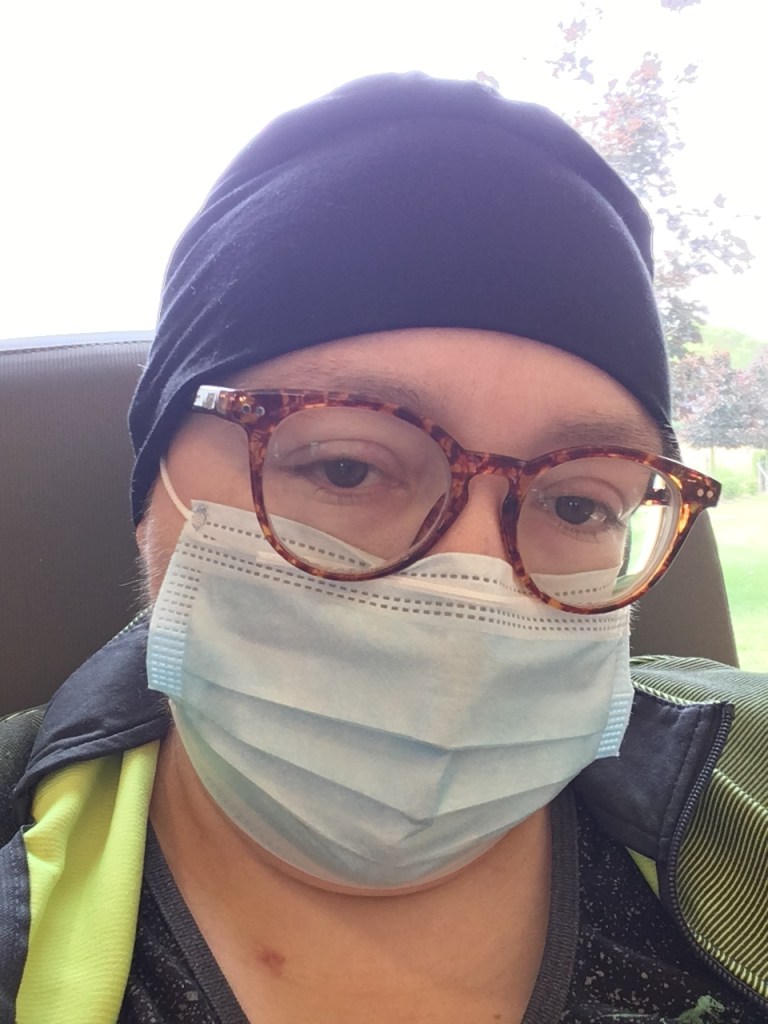
It would also be ideal if the PET-scan-results appointment didn’t take place immediately before the chemo session or other lab work because one can’t always control their reaction to bad news, and trying not to fall apart in a room full of other terrified cancer patients who are also trying not to fall apart sucks. It’s cruel for the person who receives the bad news and cruel to the ones who have to witness that person processing it. In the case of my post-chemo appointment, I was sent into the chemo room after to get my blood counts checked and my port flushed (*GAG*). I couldn’t help the tears rolling down my face. My mask mostly covered them, but my nurse and sister were close enough to see how upset I was (both were super sweet), and it hurt my heart for them to witness my attempts to keep it together.
But overall, as hard as it was, chemo wasn’t as bad as I expected.
So I guess the big question is, was chemo worth it?
Absolutely. Even though I didn’t get through chemo unscathed, for me, chemo was worth it. Sitting on my counter, I have a paper that says I wouldn’t have made it past June without treatment. It’s mid-August, and I’m still here. And my quality of life is still high enough for me to appreciate being here and to be deeply grateful.
But what has chemo cost me physically? It’s still too early to know the full cost. It can cause heart failure and lung damage up to a decade after treatment ends. It can cause secondary cancers and other ailments in the future. My lungs are damaged. I have atelectasis in both lungs and fibrosis in the lining. My lungs are adhered to my chest wall, so things like yawning hurt. Some of this was caused by inflammation, some was caused by my thoracotomy, and some was likely caused by the chemo. And it could get worse. My oxygen level stays around 95 but often dips into the low 90s, which worries me, but my radiation oncologist said they don’t worry about it until it drops to around 88. I’m also not able to stand or walk for long periods of time without debilitating lower back pain. My oncologist said this could be arthritis, triggered by the chemo. But I’m hoping that, as I walk more and more and get stronger, this will get better.
But there are also things that worry me that I thought would go away after chemo but haven’t and that my oncologists don’t have a clear answer for. One is tachycardia. Even sitting, my heart rate is usually above 100, sometimes even as high as 111-115. Minor exertion can cause my heart to shoot up to the 140s. This could be from the heart defect they found during my pre-chemo echo. Or it could be a permanent change caused by the cancer itself. I still have lymphedema in my left hand and at the base of my neck on the left side, so my left hand is larger than my right. It doesn’t cause me a lot of pain, but it’s annoying.

I also still have to sleep a little elevated, and my lungs make a bullfrog sound some mornings when I wake up. This started again before my last chemo cycle, but it’s something I went to the doctor for before the mass in my chest was found, so it caused me quite a bit of anxiety when it returned.
And I still have dizziness upon standing, which has been pretty bad today, and my feet are a little swollen, which happened only once during chemo, and not as bad as today.
So what’s next? Unfortunately, radiation therapy. Science isn’t perfect, and oncologists are often unsure and disagree with one another. As I said in a previous post, this forces cancer patients to make difficult, lonely decisions. In my case, my chemo and radiation oncologists can’t tell me if the increase in the SUV max on my latest PET scan is inflammation that will improve with time or cancer cells that weren’t killed by the chemo, but both said if the choice was theirs, they’d do radiation therapy, even with the risks (heart and respiratory failure, secondary cancers, especially breast cancer, difficulty swallowing or even loss of the ability to swallow, which can be permanent, and more). Some oncologists don’t think the risks, which are pretty high, are worth it. Others do. In my case, my cancer is aggressive and fast-growing, and when it recurs, it tends to metastasize to the brain or lungs. If it does recur, the prognosis is poor, with one study showing a 15% chance of living two years.
I recently joked on Facebook that, after being diagnosed with a rare cancer at an age when people don’t usually get cancer (NHL makes up 4% of all cancer, and PMBCL makes up 2% of all NHL, so it makes up about .08% of all cancer), whenever someone says, “But the odds of that happening are…,” I’m all like:
And yet, the odds, imperfect as they are, inform my choices. How likely am I to get breast cancer from RT? How likely am I to have difficulty swallowing? How about heart failure? What are my chances of survival without RT? In the end, though, I have to go with my gut. And my gut says, do the radiation therapy.
One of the things cancer patients have to come to terms with after a phase of treatment is that they’re not the same person they were before treatment or before cancer. Melinda Kirby wrote an excellent post about this on her blog. I don’t think oncologists do a good job of preparing people for this. This whole experience would have been easier if a doctor had told me at the beginning that I would never physically be the same person I was before cancer, no matter how successful treatment is. I will get stronger every day and be able to do more and more, but I will never be 100%. If my first oncologist had been able to be honest with me about this and the lasting effects I would most likely have from treatment and what my quality of life would be like, which would have earned my trust, the decision to start treatment would have been easier, and I would have made it more quickly. But then I also wouldn’t have found my current, awesome oncologist.
Kirby also talks about how hard post-treatment life can be, which I’m preparing myself for. Things like cancer PTSD and scanxiety can be tough, and triggers and stressors can’t always be avoided. I have to get my port removed (which I look forward to, but another procedure and round of healing is daunting). For the first two years after chemo ends, I have to get a CT scan every three months. And because I’m doing radiation therapy, I’ll have to be monitored for breast cancer every 6 months starting at age 40. And I’ll have to get routine colonoscopies and other screening tests. I’ll have to always get a flu vaccine and probably an expensive pneumonia one as well. I have a congenital heart defect that may require surgery. I might have an autoimmune disorder that may require treatment. What this means is that I’ll never really financially recover from cancer.
And yet.
I’m excited for my hair to grow back. I’m excited to start cooking again. I’m excited to be able to walk more. I’m grateful to not have to be so careful about germs (besides COVID-19). I’m grateful I made it to spring and summer and soon, fall. And I’m hoping treatment has given me enough time to see the end of this coronavirus so that my sister and I can go on trips we’ve been dreaming about. I still have my joy.

love this! you are so strong
LikeLiked by 1 person